I recently came across a paper that was published almost ten years ago (2017) but which I think is highly relevant and very interesting. But before I get into it, let me give a bit of context.
I’ve previously extolled the virtues of the “Coronary Artery Calcium” CT scan (aka “CAC scan”), which is a low-dose of radiation chest CT that looks for evidence of hardening (“calcifications”) of the arteries surrounding the heart. This scan – which can be had for about two-hundred dollars and the equivalent dose of radiation to a mammogram – does more to predict someone’s future risk for a heart attack than almost any other test we have in medicine. We continue to religiously check things like people’s blood pressure and cholesterol in medicine, which makes sense only because these are markers that help to stratify someone’s future risk for cardiovascular disease. And yet we know that these metrics are not perfect and produce many outliers (cholesterol in particular is notorious for not being that great of a predictor on an individual patient level, with many examples of people living well into their 90s with sky high cholesterol, and others of young people dropping dead with perfectly normal cholesterol). Thus while there is still value in checking such things, it really doesn’t make sense to me to do these tests but skip the CAC scan, which can much more directly measure the thing we actually care about – namely, do you have early stage/pre-symptomatic coronary disease or don’t you?
For this reason I order many CAC scans in my practice. And when a patient gets a completely normal scan, it’s an extremely reassuring moment. I can confidently look that patient in the eye and tell them that – barring a proverbial act of God – they are virtually guaranteed to not suffer a heart attack in the next decade.
(IMPORTANT ASIDE: The CAC scan is a great test for an asymptomatic person to look at their long-term risk for coronary disease. It is NOT the correct test to do if you are having any concerning symptoms, such as chest pain or shortness of breath with exercise. As always, this blog is intended as general advice, not to provide specific medical care. Speak to a doctor to discuss your particular situation and which tests may or may not make sense for you).
But what are we to do when we get an abnormal CAC result?
There are a number of tools for handling this situation. People who have coronary calcium in their arteries will benefit from keeping their blood pressure under control. They may benefit from taking a daily aspirin. If they have elevated blood sugar or other signs of metabolic dysfunction, it is extremely important that they fix that through dietary modification. If they smoke, they will gain more from quitting than from probably any other single intervention. And while I think statin medications are very overprescribed, they can be helpful in this patient population for reducing the progression of further plaque and are absolutely worth consideration, particularly in those with a very high calcium score.
But there’s another key thing that can be done for the patient who has plaque in their coronary arteries, and that is to regularly exercise. Just how powerful an effect this has is outlined in the paper I am reviewing today.
In the study, a team of researchers looked at over ten thousand asymptomatic patients who underwent a CAC scan. They also gave each patient a brief questionnaire about their exercise habits.
Then they divided the patients into separate groups based on their CAC scan results and their level of fitness: for example people with a normal scan who were highly fit, people with a normal scan who were moderately fit, people with a normal scan who were sedentary, people with a moderately abnormal scan who were highly fit, and so forth.
Finally, they followed the patients for about a decade, and charted “all-cause mortality,” meaning the very simple question of who lived and who died (of any cause, not just heart disease) over the period of the study.
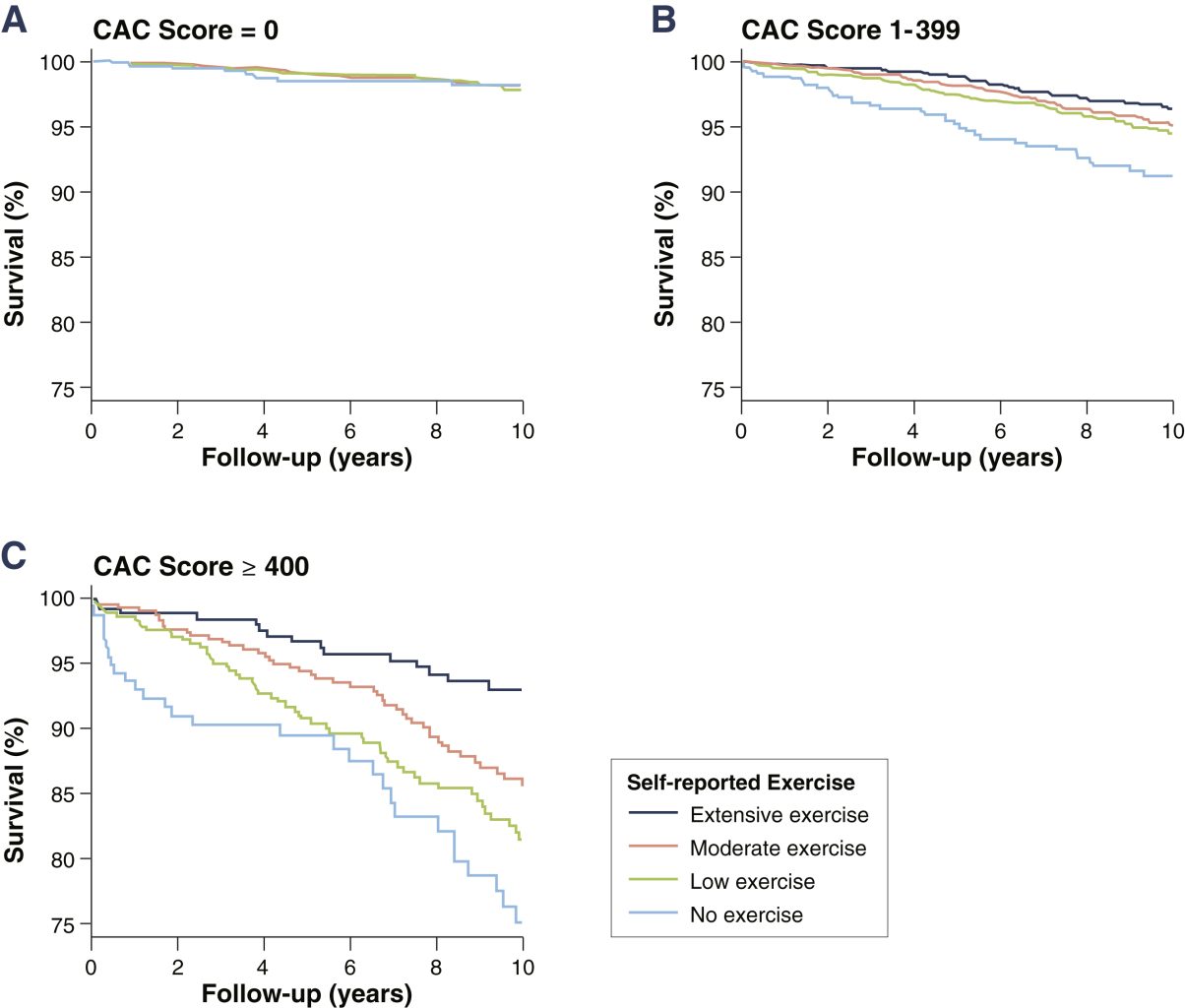
The results are best summed up visually in this graph taken from the paper:
As you can see, being an “extensive exerciser” offered a better than 95% chance of still being alive in ten years, even for those with the worst CAC scan results (Section C, “CAC Score > 400”). By contrast, more than 25% of the sedentary folks with a high CAC score died within the study period.
Of course, regardless of exercise status the better the CAC scan, the better the results (a look at Section A in the figure, “CAC Score = 0” reveals that few people with that score died, regardless of exercise status), and unsurprisingly the healthiest people had both a normal CAC scan and exercised regularly.
But crucially, even for people with dramatically bad CAC results, exercise offered massive protective benefits, not only for avoiding heart attacks and strokes, but for preventing death from any cause.
I’ve seen this in my own practice. For example, one patient I care for has a score of several thousand on his coronary scan (indicating a very high burden of coronary plaque, higher than anything shown in the graph above). Based on this score, he should be at a high risk for a heart attack. Yet to his credit, he follows a strict low-carb diet, takes his medications faithfully, and goes to the gym 5-6 times per week to do a vigorous mix of weight lifting and cardio exercise. Thus far – knock on wood – he has yet to experience any actual cardiovascular events. In fact, he’s overall in terrific shape and enjoys a level of health and vitality that most people his age would envy.
The lesson: exercise is really the elixir of youth, and it’s never too late to start.