I’ve recently returned from two weeks’ vacation in Italy, arriving home just in time to celebrate America’s 250th birthday. As of this week, the office will be back open and running as usual. Thank you to all of our patients for their understanding while we took our annual vacation.
While nobody really cares (nor should they) what a small town doctor thinks about the world at large, I’m going to use this post to just make a few brief comments about the United States on this momentous date.
We will be closed starting mid-day on June 18th for vacation, and will reopen on Monday, July 6th. Please note the following during the June 16-July 5 period:
If you are not a current patient and wish to speak with me, or if you are a patient with a very non-urgent question, please call or text me after July 6.
If you are a patient with an urgent issue, go to an emergency room or urgent care. You can text me afterwards to fill me in, and after I get back I will see you for a follow up visit if needed.
Finally, if you are a patient and have a concern that cannot wait until July 6th to discuss, but that doesn’t warrant a trip to an emergency room (for example you need a refill or a bit of routine medical advice), please text the office line and I will get back to you within 48 hours.
Recently I was doing research on xanthelasmas. Xanthelasmas are soft, yellow plaques on the eyelids that are made up of cholesterol deposits. An example is shown in the photo above. They are fairly common and completely benign. Other than being cosmetically bothersome, they do not cause any harm.
Some studies have shown they are more common in people with high cholesterol and, more importantly, that they may be an INDEPENDENT marker for heart disease risk. In other words: if two people have the same high level of cholesterol but one of them has xanthelasma and the other doesn’t, the one who has the xanthelasma may be at higher risk for a heart attack than the one who doesn’t. However, the studies on this question are conflicting, with some research showing no particular link between xanthelasma and cardiovascular risk.
I thought I would discuss this study today, not because most of you are affected by xanthelasmas, but rather because it is a good example of how medical literature can take its eye off the proverbial ball of what truly matters, and how crucially important details are often buried deep inside a paper.
If you are one of the approximately 75% of Americans who regularly drink coffee, you will probably be interested to hear about a study I recently came across. In it, doctors in Japan randomly assigned overweight adults to drink one cup of black coffee per day with the only difference being that half the participants were given coffee low in chlorogenic acids, and half were given coffee high in chlorogenic acids (I will explain what this means momentarily).
After 12 weeks, the group receiving the higher chlorogenic acid coffee had lost a little bit of weight, and crucially, shrunk their visceral fat (the type of fat that most increases the risk for diseases such as diabetes and heart attacks), whereas the group drinking the regular coffee had not. Though this a relatively small study and only lasted for 12 weeks, the results are very promising, because it was a well-done randomized controlled trial, meaning that – other than the type of coffee being consumed – there really was no difference between the two groups. They were not otherwise instructed to exercise, change their diet, or do anything else that might have led to weight loss or improved health. Hence, it appears that consuming coffee high in chlorgenic acids might lead to a little bit of weight loss and to some metabolic health improvements. You can read the full study by clicking here.
Now, you are probably thinking: what the heck is chlorogenic acid? And how can I get my hands on some? Read on.
One of my favorite movies is the very underrated Avalon, from 1990. The film tells the story of an immigrant family in Baltimore, from their arrival around the time of the first world war up through several generations, until around the late 1960s. The family is fictional and from somewhere in eastern europe (I got the sense watching the film that they were probably a Jewish family from Poland, though I don’t recall that their background was ever definitively specified), but their experience could easily stand in for millions of Americans, no matter the ethnic or religious background.
At first the family are poor and work menial jobs as they struggle to acclimate to life in America. But as the years pass and successive generations take over, they climb the ladder, achieving the American Dream of middle class affluence: better jobs, a big home in the suburbs, automobiles and televisions. However, there is a price to pay for this success, as the close family cohesion that they share at the start of the film begins to dissolve. By the film’s end, the members of the family are well assimilated into American life and much more prosperous, but also lonelier and less happy.
It’s a very beautiful film and if you take nothing from this blog post other than that you should see Avalon, then I’ve done something good for the world today. But of course, I didn’t create today’s post just to share my taste in cinema with you.
In the age of media-induced panics over every possible issue, several patients have recently asked my thoughts on the recent Hantavirus outbreak onboard the cruise ship MV Hondius. The quick punchline: I think it’s very unlikely that this will become a major pandemic ala COVID.
Here’s a brief FAQ I’ve prepared that breaks this down a bit more:
For context, the carnivore diet is an extreme version of the keto diet that shuns all plant-based foods. Followers of this diet eat only meat, fish, and maybe eggs and dairy, without any fruits, vegetables, legumes, grains, nuts, or other plant-based matter. In effect, the carnivore diet is the precise opposite of a vegan diet.
Aspirin has been around for a very, very, long time. The ancient Egyptians and Greeks used extracts of the willow bark tree – which contains salicylic acid, aspirin’s active ingredient – as a remedy for pain and fever. Then in the 1800s, chemists figured out how to manufacture a concentrated version of this substance and market it as the pain reliever we call aspirin. Right up through the 1950s, aspirin remained the most popular medication for pain, fever reduction, and inflammation. But with the advent of better medications like acetaminophen (Tylenol) and ibuprofen (Advil), aspirin’s popularity began to wane. Thus the first act in aspirin’s long story came to a close.
Before I go any further, let me just define terms here. Resistant starch is starch that your body cannot absorb. It therefore passes through the digestive tract and out into fecal waste without significant entry into the body, but in so doing it provides food for intestinal microbes, and therefore has been demonstrated to support a healthier and more diverse microbiome. Some natural sources of resistant starch include whole grains, potatoes, beans, and unripened fruit. By contrast, non-resistant starch is starch that your body absorbs and quickly converts into sugar for energy. Common sources of non-resistant starch include breads and pasta.
My kids have school break this week, so the office will be running on a very light schedule while we take a “staycation”. I’m around and available for urgent needs, including popping in to see patients as needed, but I will not be booking any routine follow ups and will not be posting to the blog this week.
As regular readers know, I’m a big advocate of exercise. I’m also non-dogmatic about the topic. Since people are much more likely to do well with – and stick to – a program they enjoy, I think it’s more important to regularly move your body in some way than to rigidly advocate for a specific program. If you love running, you should run. If you go to a yoga class that you really enjoy, you should do yoga. If you like lifting heavy things, you should strength train.
That doesn’t mean however that there aren’t specific benefits to different types of exercise, nor that you aren’t better off with a well structured approach to fitness. The “best” fitness program includes components of strength work, of mobility work, and of various types of cardiovascular fitness. If you enjoy all types of exercise and/or will stick to whatever plan is “the best” without regard for your personal preference, then a mix of something like yoga, weight lifting, and running is probably better than doing only one of those activities. But if the only exercise you will consistently do is to take long bike rides, I’d much rather you ride your bike regularly than do nothing at all because you are bored or overwhelmed by the other options.
On the topic of “the best” exercise program, I’d like to get a bit more granular today and review one question regarding exercise in particular: what is the “best” workout program to lower blood pressure.
The showing of “The Cholesterol Code” film has been rescheduled due to logistical reasons. It is now slated to be shown on Monday, May 18th, at the AMC 11 in Dartmouth, MA.
I’m on the record as stating that cholesterol is not even close to the most important risk factor for cardiac disease, that the benefits of statins are small for most people, and that there are much more important things than cholesterol to focus on for overall health. This puts me a bit at odds with the “mainstream medical establishment,” and somewhat in league with the contrarians and “cholesterol sceptics.” On the flip side, I’m also on record as stating that this doesn’t mean cholesterol doesn’t matter at all, and that I believe statins do in fact have a role to play for select patients. Which puts me in conflict a bit with the above mentioned cholesterol sceptics. To quote the late, great Gerry Rafferty: “Here I am, stuck in the middle with you.”
I started writing this weeks’ blog post about a recent article I saw in the online magazine Vox regarding the safety and benefits of statins (the most commonly used type of medication for cholesterol lowering). However, once I started writing I realized that I needed to make a major digression to explain the concept of “Number Needed to Treat”, which in turn doesn’t fully make sense until one understands the concepts of relative versus absolute risk. So I will instead make this weeks’ entry another in my series on how to read and interpret the medical literature and defer my thoughts on the Vox article to a future post.
Crohn’s disease, in case you aren’t familiar, is a type of “Inflammatory bowel disease,” in which an autoimmune process causes severe inflammation throughout the digestive tract, leading to abdominal pain, bloody stools, malabsorption of nutrients, and other serious and sometimes life-threatening complications. Like many autoimmune diseases, it has become more common over the past few decades, which strongly suggests (since our genetics have not, as a species, changed during that same time period) that environmental triggers such as pollutants, changes to our gut microbiome, stress, and poor diet likely play a role in its development.
This new study, conducted by a group of doctors in Canada, bolsters this idea. After all, if changes in the way we live can cause Crohn’s disease, then it follows that changes in the way we live should also help to alleviate it.
I have previously posted on this topic several times over the past few years – you can read my prior posts by clicking here, here, and here. Having mentioned his film and the screening it will be having in the area (April 13th at the AMC 11 in Dartmouth – click here if you’d like to reserve tickets), I’d like now to come back to this research and discuss my latest thoughts on it.
I’m pleased to announce that on April 13th, at the AMC Dartmouth Mall 11 theater (Dartmouth Massachusetts, that is), there will be a screening of the new documentary, “The Cholesterol Code.” Tickets are on sale now for the price of $22, and can be purchased by clicking here.
Beware – the theater only seats 100, so tickets may sell out soon.
For full disclosure: I am involved in promoting the film, but make no money off of it. My involvement is simply as a labor of love, because I wish to further the interesting research behind the film.
I’ve discussed this research a bit on this blog in the past, and will have more to say on it in the future, but to summarize briefly: what happens to people who go on a low-carb diet, lose weight, dramatically improve all of their metabolic markers (such as blood glucose, blood pressure, insulin levels, and inflammatory markers) but see their cholesterol rise? Does their risk for a heart attack go up, down, or stay the same? The conventional wisdom is that high cholesterol is bad, full stop, and therefore the message from mainstream medicine has frequently been that low-carb diets are dangerous due to the rise in cholesterol that some experience. However, even accepting that high cholesterol is a risk factor for heart disease, it is a much weaker one than high blood pressure, diabetes, or about a dozen other factors, so I believe the question of whether or not low-carb diets increase cardiovascular risk is a serious question and one worthy of study. The Cholesterol Code film documents research into this fascinating area and why – even in those individuals who experience an astronomical rise in cholesterol on a low-carb diet – the effects on risk for cardiovascular disease may be a lot more nuanced than we would otherwise be led to believe.
A few key points:
The film will be shown at 7:00 pm on Monday, April 13, 2026 at the AMC Dartmouth 11 theater
The film will only be shown if a critical mass of people buy tickets (65, to be precise). If you reserve tickets and we don’t hit this critical mass, you will not be charged anything, so there is no risk to reserving tickets now
Again, I have no incentive in promoting the film other than being interested in the topic. I do not make even one penny from the proceeds.
Hope to see you there. Click below to watch the trailer.
In recent years, High Intensity Interval Training (aka HIIT) has become quite popular. If you aren’t familiar with the concept, HIIT involves alternating brief rounds of very intense cardiovascular exercise with lighter activity. For example, instead of going for a light jog for 30 minutes, a person engaging in HIIT might sprint as hard as they can for one minute, then walk for one minute, and repeat the process five times for a total ten minute workout.
There are many, many, different HIIT protocols, with perhaps the most famously brief one being a “Tabata”, in which a person does intense exercise (say pedalling as fast as possible on a stationary bike) for 20 seconds, pauses for 10 seconds to catch their breath, and then repeats the process eight times for a total four minute workout.
The advantages of this type of exercise are obvious to the time-crunched person, and I indeed frequently recommend doing a “Tabata” a few times per week to the patient who tells me they have no time for exercise. There is also a psychological appeal to HIIT training for the person who doesn’t feel like they are getting a good workout unless they leave the gym soaked in sweat. Crossfit for example has long incorporated a lot of HIIT work into their programs, and if you know any Crossfitters you will be aware these are not the type of people who are content to just go for a light walk or a gentle yoga class. (That’s not a knock on CrossFit nor the people who enjoy doing it by the way – the world contains many different personality types, and it’s great to have different fitness modalities that cater to these differences. It has simply been my experience that CrossFit tends to attract the “type A” personalities of the fitness world, people who really enjoy a workout that pushes them to the absolute brink of what they are physically capable of on a regular basis).
One of the things I frequently do on this blog is to critique medical studies. There are also now a lot of blogs, youtube channels, etc. that do the same. However, the average person (understandably) really has no training on how to read or critique a medical study, so it occurred to me recently that providing an occasional post explaining some of the concepts that are frequently used when discussing medical studies might be a useful service to my readers.
Accordingly, today I will explain “power”, which is the term used to describe whether a study is or is not robust enough to detect the effect of an intervention. Let’s start with a silly example.
In last week’s post, I outlined what NAD+ is; how it declines with age and the role that plays in aging; how it can be boosted with healthier lifestyle habits; how it can also be boosted with IV infusions or by taking the oral supplements NMN or NR; and why these supplements have generated tremendous interest in recent years.
But I also explained that, at this point in time, I do not recommend supplementing with NAD+, NMN, or NR. (Needless to say, I do recommend exercise and a healthy diet, both of which have been shown to raise NAD+ levels).
Pictured: Sir Arthur Harden, Nobel Laureate and discoverer of NAD+
I have not yet spent a lot of time on this blog discussing supplements, because I think the focus of good health should be the basics: healthy diet, exercise, good sleep, stress management, and the avoidance of toxic substances such as drugs, tobacco, and excessive alcohol.
This is not to say that supplements don’t have a role, but as a category they suffer from a number of problems. They often are not backed by large and robust studies. The studies that do exist tend to be funded by companies who stand to profit from the supplement, thus introducing the same conflict of interest that “big pharma” is often guilty of with prescription medications. They are not well regulated, so even if “substance X” is truly safe and terrific for your health, you have little guarantee when you purchase “substance X” that you are actually getting “substance X”, unless you make sure to purchase from a reputable place like FullScripts (linked here in case you are interested). And supplements can give people a false sense of security – “I take a multivitamin, and therefore I don’t need to worry about eating healthfully,” or “I take creatine, so I don’t need to actually do a workout” are foolish and potentially dangerous ideas.
With that said, I get asked about this topic a LOT, so I’m going to start periodically reviewing various supplements.
First up in today’s post: NAD+ (and the supplements which help to raise NAD+, namely NMN and NR), which a number of patients have asked me about in the past few months. This is a long and complicated topic and I had to do a lot of research to get up to speed on it, so I am going to break this post into two separate parts, one today and one a week from now. But first let me just give the punchline for those of you who don’t want to read my long ramblings:
I’ve discussed in a few prior posts (for example here and here) the potential downsides of doing too much testing in medicine. This is an important topic, and one that can be difficult to discuss. Patients – quite reasonably – want to feel that their doctors are listening to them, and running all reasonable medical tests to prevent, diagnose, and treat disease. Any discussion of how medical testing can sometimes actually be detrimental to your health can therefore risk coming off as being callous and uncaring. “What do you mean I shouldn’t be tested for disease x?,” a patient may think. “Don’t you want me to know if I have it or not?” Unfortunately it’s not so simple.
I’m going to take a holiday break from posting on this blog over the next few weeks. But before doing so, I’d like to share a few parting thoughts as we wrap up the year.
A few patients have recently asked me about “liquid biopsy” tests. These are a new frontier of testing in which a single blood sample is analysed for evidence of multiple types of cancer. The idea is to analyze a single blood sample and – ideally – receive reassurance. However if you got an abnormal result, you’d then be referred for further testing to either confirm or exclude a diagnosis of cancer. This is much the same process as our current prostate cancer screening program in which a man has a PSA test as part of his annual physical to indicate the possibility of prostate cancer and then, in the event of an abnormal result, is referred for further workup (e.g. a prostate MRI or biopsy) to determine if he in fact does have cancer, or if he simply has a “false positive.” However, unlike with a PSA – which checks only for prostate cancer – a “liquid biopsy” would be able to test for dozens of different types of cancer at once.
It’s wonderful to imagine a (not so distant) future in which a blood test at your annual physical can screen you for virtually every known type of cancer (including ones for which we currently have no good tools for early detection such as brain, pancreas, or ovarian) and either give you reassurance that you are cancer free, or conversely pick up a cancer in the very earliest stages and offer a much better chance for cure.
There are a number of such tests under development (the GALLERI test from Grail, and CANCERGUARD from the makers of Cologuard are two of the better known ones), and, as you can imagine, these are igniting great interest in both doctors and patients. And while none of these tests are yet to be FDA approved – nor to be covered by any type of insurance – a few are now commercially available for those who can pay out of pocket for them. Not surprisingly then, a few patients have asked me recently whether these are worth having.
I recently came across a paper that was published almost ten years ago (2017) but which I think is highly relevant and very interesting. But before I get into it, let me give a bit of context.
In honor of this week’s holiday, I’m taking the week off from writing a blog post. A happy Thanksgiving to all of my readers and patients, and I will post something more informative next week.
To my patients: we will be hosting the holiday at our house, so I will be in the area and available all weekend for any urgent matters.
We live in a weirdly politicized and polarized time, and little better illustrates this than some of the critiques we see against the “MAHA” movement (since when did removing artificial additives from the food supply become a “conservative” issue?)
But before I get into that, I want to stress that this blog – like the practice of medicine itself – is not political. On a personal level, my politics are fairly moderate, and I have at different times in my life found myself agreeing with and voting for candidates from both major parties (and, more often, being highly critical of both parties), and I certainly have a LOT of concerns with the current administration. On a professional level, my only allegiance is to good science and good medical care. In the exam room, I am neither a Democrat nor a Republican, a liberal nor a conservative, and I’ve had wonderful relationships with patients of every political stripe over the years.
I state all of this because I don’t want what I’m about to write to be interpreted as an endorsement of any particular politician or political party. Rather, I want to highlight how reasonable scientific discussion can get dismissed as partisanship when it is offered by a politician, and to once again demonstrate just how poorly our national media does of keeping the public informed about issues of science and health.
In case you’ve never heard of it, Freakonomics is a sometimes interesting project co-founded by a University of Chicago economist and a New York Times reporter. Starting with a book by the same title in 2005, the pair have built a mini-empire of books, podcasts, and an NPR show, all examining facets of everyday life through the lens of an economist. (The original book, for example, looked at topics such as the incentives for public school teachers to sometimes help their students cheat on standardized tests, how people’s names can affect their odds of success in life, and the economic hierarchy of drug gangs in inner city Chicago).
This past week, Freakonomics had an episode on the causes of the current physician shortage. Do they do full justice to the topic? No, I don’t believe they do – but probably nobody could in just a one hour radio show. They spend a lot of time looking at the history of why we don’t have enough medical schools in the United States (certainly an important topic) and not enough, in my opinion, looking into how many work hours a typical physician is forced to waste navigating bureaucracy rather than focusing on patient care, and the generally demoralized and unhappy attitude that prevails amongst physicians, and which has led to an exodus from the field.
Nonetheless, it’s a reasonably interesting and informative episode, and if you want to know why it’s so hard to find a physician these days, you could do worse than listening to it, which you can do by clicking here:
While watching the baseball World Series the other night (what an incredible game 7, by the way! I’m not the kind of person who typically gets that drawn into watching sports, but that really was a game for the ages!), I saw a commercial that got my attention: Serena Williams, the legendary Tennis player, was advertising GLP1 agonist medication (translation: weight loss jabs such as Ozempic or Wegovy) for a company named “Ro.”
Recent headlines about a new study from Consumer Reports have created a scare about protein powders. For example, CBS has a typically alarmist opening paragraph:
Let’s leave aside the pros and cons of protein powder for this post and just grant for the moment that:
a) people can get all the protein they need from a well balanced diet and don’t need protein powders, and b) some people, for a variety of reasons, find benefit to including protein powders in their diets.
For those who fall into this later category, should they stop using protein powders simply for fear of lead contamination?
In my last post, I fleshed out some of the logical arguments for why overtesting (the practice of ordering lots of tests, “just to check”) can sometimes backfire on patients and lead to worse outcomes. Today I’m going to provide brief vignettes of two actual patients I cared for during my residency training to better illustrate the point.
Many people assume that the lack of pro-active testing for every possible problem in medicine is simply done as a cost savings measure. Patients will sometimes complain to me that their insurance won’t cover a periodic full-body MRI, or a routine stress test, or blood testing in the absence of any symptoms for this disease or that. And there is some validity to this critique: it’s certainly true that insurers like to spend as little money as possible on patients. But to be fair, there is another side to the argument, which is that – contrary to what many assume – testing for problems that aren’t apparent can sometimes in fact be harmful.
This is a difficult topic to grasp, so I’m going to break this post down into two parts. Today, I will outline some of the logic behind why tests can sometimes create more problems than they prevent. In next week’s post, I will give a few actual anecdotes from my career that demonstrate the point.
How could it possibly be that ordering tests to screen for health problems can be harmful?
The researchers in the study performed several separate lines of research and published them all in one paper. First, using advanced lab techniques, they studied humans and determined the following:
I don’t think I’ve mentioned it before, but one of my favorite health podcasts is called “Zoe.” Zoe is a British-American company that offers a service of personalized testing: they mail you a kit so you can submit a blood specimen and a stool specimen, as well as wear a continuous glucose monitor for a few weeks. Then they analyze all of this data and come up with personalized nutrition recommendations for you that are supposed to best sync with your own biology. I have no idea whether this works well or not, but the podcast that they use to market their product often features great conversations with legitimate scientific experts.
At any rate, I enjoyed their latest episode, which covers a subject near and dear to my heart: how to sleep better. Included in the episode are some of the topics I hammer home a lot (such as having a steady wakeup time, getting morning sunlight, and developing good beliefs around sleep), as well as some new tips and tricks that I was not previously familiar with. If you’d like to give the full episode a go, you can listen to it here:
Pictured Above: Max Liebermann – “Beer Garden near the Havel under Trees”, 1920
No, I’m not going insane. I’m just using this week’s blog post to engage in some stream of consciousness. So this post will be long and wandering, but I promise – I do have a point or two to make.
Regardless of where you stand politically, the recent assasination of Charlie Kirk was the latest in a string of public violence which should raise alarm bells about why so many Americans have become socially isolated, mentally ill, and radicalized by the internet into holding profoundly anti-social views. (I’m thinking not only of political assassinations and attacks, such as the slaying of several Democratic lawmakers in Minnesota, the attack on Nancy Pelosi’s husband, or the two failed assassination attempts on Donald Trump last year, but also of the all-too-frequent school shootings and mass terror attacks in this country).
Here’s a quick review of an older study (from 1997). In the study, they took middle-aged diabetics and randomized them to do either nothing, or to do 45 minutes of vigorous cycling on a stationary bike twice per week, plus one session of high-intensity interval cardio training (consisting of two minutes of vigorous exercise followed by three minutes of light exercise for five cycles, for a total of 25 minutes).
After two months, the people who did the exercise had lost 48% of their visceral fat, and significantly improved their insulin sensitivity and blood glucose numbers, even though they didn’t lose a significant amount of weight overall. You can read the full study by clicking here.
This post is an informational reference for current patients of mine. While the general public is welcome to read it, the specifics of the following applies only to my current patients:
One of my goals in starting Dr. Fischer, MD, was to be able to break free of the restrictions of insurance driven medicine and offer my patients what I believe is the best care. In this vein, I am excited to announce that we will be holding a screening clinic for esophageal cancer on the afternoon of Tuesday, October 28th.
Esophageal cancer has become much more common over the past few decades, and is often deadly. Now a new technology, called Esoguard, has been developed and approved by the FDA. Esoguard is able to detect pre-cancerous changes in the esophagus years before they would go on to be a problem. I believe that in the future this technology will be widely used in the American medical system, but right now most insurers have not gotten around to approving it, and it will be a long time before this technology is standardized and deployed widely at more traditional medical offices.
However, I am excited to announce that – for my patients who qualify – this technology is available now, at no out of pocket cost.
If you are a current patient of mine who is interested in learning more, please read the rest of this very carefully.
This post is just for fun, and light on science. So if you’re looking for something firm to hang your hat on, skip it. On the other hand, if you want to be bored by my personal thoughts, read on.
Today, I’d like to briefly return to this topic by discussing how the ancient Romans ate. But before doing so, I want to make two points:
The ancient Romans lived, on average, much shorter lives than we do. So it’s not that we should copy their world completely.
But as the old saying goes, there are “lies, damned lies, and statistics,” and in point of fact a major reason that average life expectancy in Rome is estimated to have been about 30 years is that roughly half of all people in the Roman empire died in childhood. Of those who did survive to adulthood, many young women died in childbirth, and many young men died of traumatic injuries (being a Roman soldier, or building aqueducts by hand, turns out to have been dangerous work). As a result, an enormous percentage of the population died at a very young age, which brought the average life expectancy down considerably. But of those who didn’t die young, many went on to live a fairly full life, and in point of fact quite a few Romans lived into their 60s, 70s, and 80s. And while we have no way of knowing exactly what happened to these folks, there are many lines of evidence to suggest that they suffered less than we do from obesity, diabetes, cancer, heart disease, or dementia. The point being, there might be some things these ancient folks can teach us about how to age well, despite the fact that the majority of them never got the chance to.
Secondly, I am using Rome only because it is such a cultural touchstone of ours, but there’s nothing unique to Rome in what I am discussing. Substitute in any other pre-modern civilization – the Persians, the Ottomans, feudal Japan, or whomever you choose – and you could likely draw a lot of the same insights.
If we think about this pattern, we’ll note a few things. Firstly, that it contains no processed or packaged foods (duh). Secondly, the diet is high in fiber and plant matter. Third, it is low in sugar (in fact the Romans didn’t have table sugar the way we do, though they did eat fresh fruit and honey to satisfy their sweet tooth). Fourth, it contains a fair amount of fermented foods (sourdough bread, cheese, wine), which we now know helps to nurture a diverse and healthy gut microbiome. Fifth, it is not per se low fat, but it is low in saturated fats and, of course, is completely devoid of the industrial and processed oils that are common in the modern western diet.
In fact, if we examine the above diet, we’ll note that it is pretty consistent with the dietary pattern that modern nutritionists call the “mediterranean diet,” still followed in many parts of Greece, Italy, Spain, and other mediterranean countries, and which numerous studies have shown is a healthy eating pattern for reducing the risks for obesity, diabetes, and cardiovascular disease.
Therefore, one way to look at healthy eating patterns is that they are something to be discovered by modern scientists. But another is that they are something to be re-discovered from our pre-modern ancestors who by a mixture of intuition and limited options (Burger King, sodas, and packaged chips just weren’t available to anybody living prior to a few decades ago) tended to follow, at least in some regards, a healthier eating pattern than we do.
One suggestion I often give my patients is to forget for a moment about fat, calories, protein, etc, and simply try never to eat a food that didn’t exist a century ago. If you follow no rule other than that, you will likely have a healthier diet than about 90% of modern Americans.
Gratitude to my wife (and office manager) for sharing this interesting study, published in 2022, with me.
Researchers at Penn State University randomly assigned 235 post-menopausal women to either eat 50 grams of prunes (aka dried plums) or not every day for a year. For context, 50 grams of prunes is about six prunes per day. After a year, they found that the women eating the prunes had better bone mineral density, and an accordingly lower estimated risk for bone fractures, than the women who weren’t.
In other words, doing absolutely nothing other than adding six prunes per day to your diet might be a tool to keep your bones healthy, at least in post-menopausal women.
Please be aware that the office will be closed during the weeks of August 11th and August 18th for summer vacation. We will be re-opening on Monday August 25th.
If you are a current patient and have an urgent medical concern, please go to the nearest emergency room or urgent care center. You can reach out to me afterwards with a text message, voicemail, or email to update me on things so that I can follow up with you upon my return.
By contrast, if you are a current patient and need to reach me for a non-urgent issue such as getting a refill or discussing a minor medical problem, you can text or email me and I will get back to you, but there may be a delay of 24 hours or so as we will be traveling abroad.
Thank you for your understanding, and I hope you are having a nice summer.
In the study, the famed Dr. Dean Ornish (who is best known for a 1990 study that used a similar intervention to reduce heart attack risk) at the University of California San Francisco took patients with early-stage dementia and divided them into a control group (who didn’t do anything in particular) and a study group who received an intensive lifestyle intervention that consisted of:
A low-fat vegan diet
Regular meditation and yoga for stress reduction
Daily “cardio” type exercise
Prioritizing good quality sleep
The results after 40 weeks were that the people in the control group got worse (as expected), whereas in the people receiving the intervention, 46% improved and 37% stabilized on a series of cognitive tests. Put another way, 83% of people doing the lifestyle program did a lot better than the people not doing the lifestyle program.
This is yet another example of what I have termed the “Academic-Media Complex,” in which bad studies are given hyped up reviews by the media, leading to more funding for research universities and more sales/clicks for news organizations, but poor information for the public.
If you read the original study (which you can by clicking here) the results are – shocking, I know – hardly what they are hyped to be.
I haven’t written yet about the new weight loss medications that are sweeping through society (Ozempic, Wegovy, Mounjaro, Zepbound, etc) but that’s not for lack of experience with them. Patients frequently ask me about these medications and yes – I do sometimes prescribe them. Given that interest in these medications is only growing, I thought it was about time to create a blog post on the topic.
There is already a severe shortage of primary care doctors in the state
A third of the primary care doctors who are currently practicing in MA are approaching retirement in the next few years
Very few young doctors are entering the field to replace those retiring doctors
Hence, the shortage of doctors is going to get much, much, worse over the next few years.
The article discusses a proposal called “Primary Care For You” that would attempt to rectify the problem. Unfortunately, while it’s certainly a good thing that somebody is paying attention and at least trying to remedy the crisis, I’m not very optimistic from the reporting in the article that this plan will make much of a difference.
Recently, a patient asked me what I think of the tap water here in Marion, noting that many of her friends refuse to drink it, and choose instead to drink only bottled water.
In fact, I had the water at my house tested by a private company a few years ago, and the report came out quite favorably. (I don’t recall the name of the company that did it, and have no endorsement of a particular company in this regard). I think getting the water in your home tested periodically is not a bad idea for anybody to do. It’s also possible to get a good quality water filter for your home if you want to ensure the purest water possible. Again, I have no particular brand to endorse in this regard, so if this interests you, do your own research.
What I do wish to specifically comment on today is how awful bottled water is for you.
A theme I come back to over and over again on this blog is the benefits of a simple exercise regimen that requires minimal time and equipment. Building on this theme, I’d like to briefly post today about one of my personal favorite exercises: the farmer’s carry (and its one handed equivalent, the suitcase carry).
I’m excited to share that, as of last week, I am now licensed to practice telemedicine in Florida. I took the step of obtaining this extra license because I have a number of patients who spend part of the winter in that particular state, and it seemed like it would be useful to be able to dispense health advice (not to mention medications!) via phone or Facetime without having to worry about running afoul of medical licensing laws.
As my patients – and regular readers of this blog – know, one of my frequent recommendations for better health is to increase the intake of dietary protein. Dietary protein is satiating, which tends to lead to lower overall caloric intake, and thus less fat mass. At the same time, dietary protein supports muscle mass, particularly when combined with a regular program of physical activity. The combination of less fat and more muscle leads to lots of desirable outcomes, from improved health (lower blood pressure, lower blood glucose, improved metabolism, lower risk for frailty with aging) to a more visually appealing body aesthetic. Does this strategy work for everyone? No, we’re all unique. But for a lot of people it’s quite helpful.
However, frequently when I make this recommendation to patients, I am met with one particular concern: “won’t all of that extra protein harm my kidneys?”
Last year, I provided a link on this blog to a lecture I gave in 2023, about how lifestyle changes can improve arthritis and other musculoskeletal pains. If for some reason you want to watch that lecture, I will link to it here.
But to give you the brief summary of what I covered in that talk: being overweight doesn’t just cause arthritis by increasing physical pressure on the joint, but also because fat cells have the effect of up-regulating inflammatory signals in the body, which in turn lead to weakening of muscle, increased pain receptors, and other factors that create more pain.
Now a new study published in JAMA supports this point.
I’ve blogged on many occasions about my frustration with our national response to type 2 diabetes. While type 2 diabetes can be dramatically improved, and often outright cured, with lifestyle interventions such as diet and exercise, our system instead treats it as an intractable chronic illness that can merely be managed, not banished. Millions of patients are immediately put on medication at the first sign of poor blood sugar control, and while they are typically given some lip service about eating more healthfully, exercising, and losing weight, the focus of their treatment over the ensuing years involves an ever expanding pharmacopeia of medications. There is certainly evidence that many of these medications do help when compared to doing nothing, but it’s clear that even well treated diabetics don’t live as long and full lives as non-diabetics. So to me, this medication-centered approach is a tragedy of epic proportions.
Last year, I blogged in two separate posts about research into the topic of heart health and the keto diet. Now a follow-up study on this research has been published which sheds some important light on the topic.
Before getting into this new research, it would be worth your time to read (or re-read) my two prior posts on this topic, which can be found by clicking here and by clicking here.
A topic that I love, but haven’t yet gotten to comment on on this blog, is the remarkable health benefits of sauna use.
Over the past few decades, a large body of scientific research has shown that brief exposure to temperature extremes (both hot and cold) can lead to some biochemical processes in the body that promote better health. In a way, this is analogous to intense exercise. During a bout of intense exercise (say, doing sprints or jump ropes), certain chemical processes are upregulated in your body. In the hours after you finish exercising, these processes lead to beneficial effects in your body such as lowering your blood pressure, slowing your resting heart rate, and improving your insulin sensitivity. Similarly, being exposed to 15 or 20 minutes of uncomfortably hot air can lead to changes in your body over the ensuing hours that are beneficial to health.
One of the popular strategies for weight loss over the past decade has been intermittent fasting, or as some researchers call it, time restricted eating.
In case you don’t know what this is, it’s simply setting a restricted schedule around when you eat and when you don’t. Studies have shown that the typical American spends more than 15 out of every 24 hours in a “feeding” state, meaning that they eat shortly after waking in the morning, and then consume multiple meals and snacks throughout the day right up until shortly before bedtime. As a result, the longest stretch they ever go without eating in a typical day is no more than 9 hours, most of which consists of the time they are asleep overnight.
By contrast, somebody who is intermittent fasting might follow one of the following schedules:
In my last post, I talked about the importance of maintaining humility when promoting or dismissing lifestyle interventions for better health. Today I’m going to flesh that out a bit further.
There’s an old joke among epidemiologists that goes like this:
The Japanese eat very little fat and suffer fewer heart attacks than the British or Americans. The French eat a lot of fat and also suffer fewer heart attacks than the British or Americans. The Japanese drink very little red wine and suffer fewer heart attacks than the British or Americans. The Italians drink excessive amounts of red wine and also suffer fewer heart attacks than the British or Americans. The Germans drink a lot of beer and eat lots of sausages and fats and suffer fewer heart attacks than the British or Americans.
Conclusion: Eat and drink what you like. Speaking English is what kills you.
Today’s post will just be some musings of personal observation.
If you follow any online “health influencers,” you will notice that they often attract a rather passionate set of followers and detractors. For example, you will commonly find influencers in the low-carb community (and their followers) denigrating anybody who disagrees with them as not just wrong, but as stupid or corrupt. I commonly see commentary around such influencers that doctors have “lied to” the public about sugar; that the data linking high cholesterol to heart disease is based on only a few flawed studies from the 1950s; and that Ancel Keys (one of the early leading proponents of reducing saturated fat and cholesterol) made up his research results – none of which is true.
On the vegan side of things, one can find the same tendencies. I’ve seen interview clips of Michael Gregor (a prominent vegan physician and author) for example promoting the idea that a vegan diet is the “only” diet shown to reverse heart disease (it isn’t). And as a resident I once took care of a patient in the hospital who refused to believe – despite all evidence to the contrary – that she had had a heart attack, because she was a vegan and “if you don’t eat animal products, you can’t get heart disease.” (In fact, cardiovascular disease is the number one killer of all Americans – vegans included).
A recent study out of Northeastern University (just up the road from here, in Boston) makes a point that I harp on a lot: you can go most of the way toward meeting your fitness needs without any gym membership, without any fancy equipment, and without leaving your home.
I’d like to use this post to introduce a very simple, and important, concept that is a key idea to understanding metabolic health: the “personal fat threshold.”
Before doing so, I just want to clarify my point of view about this: I am not suggesting that butter is a health food, nor that you might not be better off eating less of it. The balance of the evidence, for example, strongly suggests that good quality olive oil is much healthier for you than butter. So please don’t read this post and walk away thinking that butter is unambiguously good for you and that the more of it you eat the better, as is promoted by some health influencers on the internet.
Time for some inspiration. Last year there was quite a bit of media coverage about one Richard Morgan, a 93 year old Irish man who is a champion indoor rower. Scientists analyzed Mr. Morgan and found him to have the cardio-respiratory fitness of a man half his age. The reason this is so amazing is that Mr. Morgan didn’t take up any exercise at all until age 73, after he retired from his career as a baker. And while it’s impossible to ever draw broad medical conclusions based on one-single case, his story certainly lends credibility to the idea that it is never too late to start getting into better shape.
In my last post I covered a new line of research about possible post-vaccine harms, and how it has been sensationalized and misrepresented in the media. Today I want to step back and more broadly share some personal thoughts on COVID and on the vaccines.
I haven’t commented on the vaccines nor on COVID before, and I have a lot to say on the topic. So I am going to split this into two posts. Today I’m going to deal with the above article only; in my next post I will give you my thoughts more broadly on COVID and on the vaccines, as somebody who worked on the “front lines” during the COVID pandemic and has experience treating thousands of COVID cases.
I’ve written at length on this blog about the benefits of regular physical activity and a simple approach to staying fit that doesn’t just rely on “working out.” To highlight this point from a different angle, I want to revisit a study that is now a quarter-century old.
I discuss nutrition a lot on this blog, and two themes I come back to over and over again are the importance of avoiding processed foods and the benefits of increasing protein. I’ve also stated in the past that I am diet agnostic, by which I mean I believe a multitude of diets can work and the most important thing is to find the diet that works for you. With that said, patients and readers of this blog may have picked up on the fact that I tend to be partial to low-carb diets. This is not because I believe that low-carb diets are the only way to lose weight or that they are always the best choice, but because in my years of practice I’ve found many patients to have an easier time sticking to these plans and therefore achieving results than they do with other types of diets.
Where do plant based/vegan diets fall into my thinking?
Last week marked one year since Dr. Fischer, MD, first opened its doors. Starting with just a single patient, we have since grown to almost 140, with new patients signing up every week.
Coming from a practice where I had over 2,000 patients and spent much of my time doing paperwork for the insurers, I have rediscovered the joy of practicing medicine in an environment where I get to spend an hour or more on patient visits, make housecalls, implement a more holistic and preventative approach than our insurance run “sick-care” model allows for, and have time to take an actual lunch break most days.
A heartfelt thank you to the patients who have made our practice successful. I look forward to working with all of you for many years to come.
Emergency hospital during influenza epidemic, Camp Funston, Kansas (1918). Original image from National Museum of Health and Medicine. Digitally enhanced by rawpixel.
I’ve seen a lot of viral illnesses the past six weeks or so: COVID. Bronchitis. Sinusitis. And of course, the flu. This is the time of year when people get sick with all kinds of sniffles, sore throats, coughs, chills, and aches. Understandably when people are sick, they want to get better as quickly as possible. Ergo, many patients who test positive for flu will ask me for Tamiflu.
My last post discussed the importance of building muscle for good health and slower aging, and how this in turn requires regular strength training (such as lifting weights, though that is not the only modality for achieving muscle health) and adequate protein intake.
Before moving on from this topic, I want to take a moment to give a special emphasis on this point to any female readers of this blog.
One of the concepts I spend a lot of time talking to my patients about is the importance of maintaining muscle health. The reason for this is that virtually all people start to gradually lose muscle beginning somewhere in their 30s or 40s. At first these changes are barely noticeable, but by the time they are in their 70s many people will experience a huge degradation in their degree of fitness.
This coming Monday, I will be giving a brief talk at the Marion Council on Aging entitled “How To Become a Better Sleeper,” which will piggyback off of my prior series of posts on the topic. The talk should be about half an hour long, with some time for Q&A afterwards. If you are in the area, please feel free to drop in.
Happy New Year! This is the time of year when many people make resolutions, with getting fit being amongst the most common. Of course, research shows that most people quit their new year’s resolutions by around March. So this year, I’d like to suggest you take a different approach: rather than giving yourself overly ambitious goals in the gym, instead learn to bake some very modest but high-yield habits into your life.
While this may not sound as sexy as committing to some kind of “beach body” program, the fact is that with exercise, a little goes a long way. A very long way. To this end, I’d like to highlight two threads of research for you.
Merry Christmas, Happy Hanukah, and Happy New Year to all of our patients.
I will be taking the next few weeks off of writing this blog (don’t worry – I’ll still be in the office seeing patients on a limited holiday schedule, and of course I’ll still be available to any of my patients who have urgent needs come up) to wrap up the year and spend some time with family over the holidays.
Wishing you and yours a safe and happy holiday season, and I’ll be back with more to say in 2025.
One of the tools that I’ve gotten more interested in the past few years are Continuous Glucose Monitors (aka CGMs). These are patches that can be painlessly applied to the arm and that sync to an app on your phone, providing continuous information about your glucose levels. While they are not 100% accurate, they are close enough to more traditional methods for checking glucose (e.g. fingerstick) to give a pretty close estimate of your blood glucose at any particular moment, and since they can provide hundreds or even thousands of data points per day, can be used to track trends and see patterns.
Dr. Means trained as an ENT surgeon at Stanford University before deciding that our current profit driven sickcare model was the problem, not the solution, for most of the issues she was treating, and that she would rather serve patients in a different capacity. This led her to become a functional medicine practitioner, and later to help found the company Levels, which uses continuous glucose monitors to help people glean insights into their metabolic health and learn how to make improvements therein. Now, she’s written “Good Energy”, which has been on the NY Times bestseller list for the past few months.
If, like me, you came of age in the 1980s and 1990s, you probably don’t remember a time when you weren’t warned to stay out of the sun. The message for the past few decades has been that sun exposure = skin cancer, and that if you absolutely have to go out during daylight hours for more than a nanosecond, to please not do so without first donning sunscreen and a full suit of body armor.
It’s true that excessive sun exposure can cause skin damage and increase the risk of skin cancers. But there’s (pun intended) a wrinkle to this. And that is that limiting sun exposure might also increase your risk of getting lots of other diseases, including heart disease and virtually every other known cancer. I’ll discuss some data about this in a moment, but first I want to just share some thoughts about sun exposure in general:
This post will be short. It’s Thanksgiving week and I want to wish all of our patients and readers a very safe and happy holiday. Though the office will be closed for the long holiday weekend, we are hosting family here in town and I will be around, so to all of my patients – I am available both by phone and in person if something urgent does come up.
Rather than just leave things at that, I’d also like to do something here that I’ve been meaning to do for awhile: post a link to a series of articles I wrote under an assumed name a few years back. At that time, I was employed by a large group practice and didn’t want to say or do anything that could put any of my partners in a difficult situation, so I wrote these under the name of “Reginald Bittermilk.” But since I now work independently, I no longer feel that restriction.
I wrote these articles at the request of a friend who wanted to publish a series of essays about what is wrong with America’s healthcare system from a doctor’s perspective, and what some possible solutions might be to fix things. If you find dealing with a mainstream doctor’s office to be frustrating, I hope this series will give you some insight into why the system is so broken, and some empathy for the challenges that doctors and nurses face every day in trying to deliver good care to their patients. When you need a break from your family this coming holiday weekend, you can read the series of articles at the following link:
This is not because I have anything against supplements per se. Some in fact have good evidence for them and can be quite beneficial. But it’s rare that a supplement is the most important part of the healing process, and often they are a band aid of sorts for something else that is going wrong in a patient’s life.
When my wife and I opened Dr. Fischer, MD on February 6th of this year, we had just one single patient. This past week, we signed up our 100th patient. That’s 100 patients in just nine months.
When we first opened, many people asked me how we could possibly be successful with this business model. I was very confident we would be, but of course you can’t know for sure if something is going to work until you actually try it. Well, we’ve tried it, and here are a few facts:
The consultant who helped us set this practice up (and who was also very confident we would be successful) projected that we’d be at about fifty patients at this point. We are now at double that amount.
We are already profitable as a business
In roughly another forty patients, I will match what I was earning at my last job
If you are a fellow physician thinking about setting up a practice like ours, my advice is to get off the fence and do it. You won’t fail. And feel free to reach out to me if you’d like to ask any questions.
If you are a patient who is thinking of checking out our practice, don’t delay scheduling your free meet and greet. At the rate we are growing, it will only be a few more months before we have to slow down the number of new patients we can take on.
Finally, a heartfelt thank you to all of our patients who have made us a success. It’s a true honor and privilege to be entrusted with your medical care.
This blog post is going to be a little different than usual. I’m not going to cover a study or discuss a particular medical topic. Rather, I just want to share some personal thoughts on this political moment.
I am not going to endorse a particular candidate, nor a particular set of policies. Like any other citizen, I have my thoughts and ideas about this stuff, and I will be voting today for my preferred (or, more accurately, my less non-preferred) candidates. But as a doctor, I am meticulously non-partisan. I take care of Democrats and Republicans and anybody else equally, and it’s my job to stay out of the political fray and do my absolute best for each and every person who comes to me. I took an oath when I entered this profession, and that was to serve my patients to my utmost. If a person whose politics were truly loathsome showed up at my office (let’s just imagine Adolf Hitler himself, to make the point clear), I would still do my very best to help them with their medical issues.
I’ve been meaning to review this study for some time now. A few years ago, a cardiologist at the University of Texas by the name of Dr. Ben Levine conducted a study that ought to be on the minds of anybody who is interested in living a longer and healthier life.
Dr. Levine and his colleagues put middle aged adults (around age 50) who were previously sedentary but otherwise healthy on an exercise protocol for two years, and performed various tests on their hearts before and after the study. They found that after two years, the subject’s hearts had effectively reverted back to those of a 30 year old’s. In other words, exercise made these people’s hearts age in reverse by almost twenty years.
In my last blog post, I took the New York Times to task for incorrectly suggesting that new research demonstrates a connection between alcohol consumption and the rise of cancer in younger adults. And then just a few days after I wrote that, a patient asked me my thoughts on the health risks of alcohol. So I thought I’d dedicate a post to the topic.
Let’s start with a simple fact: alcohol is toxic to the human body. There is now a lot of research to suggest that even moderate alcohol consumption may play a role in the development of some cancers and in neurological disease. It’s also well established that alcohol consumption is tied to an increased risk for atrial fibrillation, a common type of heart arrhythmia that can increase the risk of having a stroke. And the longstanding belief that moderate alcohol consumption is protective against cardiovascular disease has not held up under closer scrutiny. No, one glass of red wine per night will not cut your risk for a heart attack, and wine consumption is not the reason that countries like France, Italy, and Greece have lower rates of heart disease than we Americans do.
Add to this the long established fact that heavy alcohol consumption is terrible for the body, and substantially increases the risk for liver, cardiac, and brain disease, and we can reasonably conclude that alcohol is bad for humans. Period, full stop. And looked at purely as a substance examined in isolation, this is a correct conclusion. However…
Recently I watched the documentary “Hack Your Health,” which is available for streaming on Netflix. The film covers the emerging science of the gut microbiome (the population of trillions of bacteria, most either harmless or beneficial to human health) that live inside our GI tracts, and that are increasingly being found to play a role in everything from our tendency to gain weight, to our mood, to our risk for various chronic diseases.
I really wanted to like this film, because I think the gut microbiome is a fascinating and important emerging area in medicine, but the film suffered from some major flaws. Overall, I’d give it two out of five stars.
The photo above is one I took during my recent vacation to Germany. While stopping to tour a beautiful church in a picturesque small Bavarian town, we wandered into the adjacent cemetery and stumbled upon the gravestone of this local legend, who lived (in the 1700s, before modern medical care!) to the ripe old age of 117. I’ve been thinking of Herr Adner lately, because here in 21st century America, things are looking less rosy. After two centuries of unabated progress, in which the health and longevity of Americans slowly but steadily improved, Americans as a whole are getting sicker and dying younger than they were just even a few years ago. In 2019, the average life expectancy in the US was 79; now it’s down to about 76.
I met a new patient recently who was quite concerned about his cholesterol after his last doctor suggested he go on a statin. After discussing this patient’s medical history and reviewing his labs, it became obvious that he does NOT have a cholesterol problem, and certainly not one that warrants medication. This is a common scenario I run into in clinical practice, so I thought it would be useful to take a few minutes to run through some of the thought processes that a doctor should take when evaluating a patient’s cholesterol.
Without further ado, let’s delve in. Here are a few key points that are important to understand when thinking about cholesterol. Read through them, and then I’ll come back to the patient.
In my last post, I reviewed some of the background on how and why cholesterol came to be viewed as a risk factor for heart disease, and how this creates a clinical conundrum for those who go on a low-carb diet and see a big rise in their LDL (the “bad”) cholesterol but see every other aspect of their health improve. I discussed how there is a paucity of research on this particular population of patients and, hence, a lot of controversy about this topic. Then I introduced the work of Dave Feldman, a software engineer and internet personality who has been leading a grass roots research effort into this very topic. And I reviewed how Dave has proposed that maybe – just possibly – the metabolism of people on low-carb/keto diets is so different from that of a person following a more typical diet that cholesterol simply doesn’t behave the same way in their bodies, and hence the research we have until now suggesting that high cholesterol is a risk factor for heart disease might not apply to them.
I’m going to spend the rest of this post discussing a fascinating study that Dave and his colleagues just published which attempts to shed some light on this question. But first, let me stress that all of this remains theoretical, and – spoiler alert – we still do not know if having severely high levels of cholesterol due to a low-carb/keto type of diet is safe. One study does not a fact make, and most doctors would advise continued caution in this area. And while I do feel that the obsession on cholesterol and its treatment has had some real downsides (by emphasizing a laser focus on this one risk factor, while far more important risk factors such as metabolic syndrome/insulin resistance get ignored), it’s only fair to admit that there are still many, many, papers out there showing that – on a population level – there is a strong link between elevated cholesterol and cardiovascular disease risk. Please keep that in mind as you read the rest of this.
I’ve spent my last few posts focusing on some very bad studies that have been prominently featured in the media lately. Now I’d like to discuss a recent study that has gotten less attention, but that I think is far more interesting and useful. However, before I get to the study itself (in the next post), I need to go into some background.
A patient recently brought this study to my attention: as reported in the journal Nature Metabolism, high protein diets apparently lead to heart disease. Or, as the New York Post put it in their headline:
At the risk of sounding like a broken record, this is another example of the “Academic-Media Complex” that I often warn about, in which a terribly designed study that tells us nothing about human health is reported on in sensational terms by our “if it bleeds, it leads” media.
Not too long ago, I had a post (link here) about the fact that much of what is published in the medical literature are very poor quality studies, and the symbiotic relationship between academia and the media that hypes these studies up, thus sewing fear and confusion into the average person.
I really can’t stress this point enough. It’s not that most medical studies are good, with a few poor ones thrown in. It’s that a large percentage of what is published and reported on in the news sheds absolutely no light at all on how you can live a healthier life, and is often frankly misleading. So it’s a point worth revisiting over and over.
I just returned from vacation, and after an eight hour flight home, my lower back has been a little sore this week (thank you Lufthansa for the cramped seats!) Which got me thinking about the topic of low back pain, and that I have yet to comment on it on this blog.
Back pain is one of the most common conditions we see in adult primary care. It is also one in which the western model of medicine really falls down. To explain what I mean by this, let’s consider two other common diseases, and then consider back pain:
We will be closed for summer vacation from now until August 20th. Please note the following:
We will be traveling without perfect internet connection, so we will not be able to respond to messages on an urgent basis. If you are a current patient and are having an urgent issue, go to the nearest emergency room or to an urgent care center. You can leave us a message later telling us about it so that we can arrange any needed follow up as soon as we return.
If you have an issue that can’t wait for our return but isn’t an emergency (for example you need prescription refilled or you have a minor medical issue that you need assistance with), call or text the office and leave a message, and we will get back to you within 1-2 days. We also do have a trusted colleague who can see our patients for an in person visit for non-emergency issues, and if you indicate the need for such in your message, we can connect you to him.
If you are not currently a patient of ours but are interested in learning more about the practice, setting up a free “meet and greet” for after our return, or enrolling as a patient, you can still call the office and select the appropriate phone option. We have an outside business consultant who assists us with new patient inquiries, and she can field these calls on our behalf and assist you even in our absence.
Thank you for your understanding while we travel, recharge, and spend some time with our kids. We hope you are enjoying a happy and healthy summer.
In this election year, we are likely to hear politicians from both major parties blather on about their preferred solution for “healthcare.” I can accept that intelligent people, acting in good faith, can come to very different conclusions about how our system should be run in the United States, but what drives me crazy is how the very parameters of the debate indicate muddled thinking and an inability to clearly articulate the nature of the problem. So let me take a moment to briefly define three different terms that are often used interchangeably, but shouldn’t be, and then talk for a moment about why this matters:
Health insurance is a mechanism by which we pay for healthcare. It is important to understand that it is NOT in and of itself healthcare.
Healthcare is the actual provision of health services to a patient. Healthcare consists of things like doctors, nurses, medications, tests,hospital beds, and surgical equipment.
Health is the absence of disease. A person who possesses good health will need little in the way of healthcare.
It’s crucial to keep the distinction between these three terms in mind as we think about our broken healthcare system. Our politicians talk endlessly about the need to reform “healthcare” or provide “healthcare for all,” or whether “healthcare” should be a right versus a privilege, but what they are really talking about is health insurance, NOT healthcare.
Direct Primary Care (DPC) is really so different from the sort of corporate medical practice that I spent the first decade of my career in (and that most patients are familiar with) that at times it’s hard to convey to prospective patients just how different their experience can be at an office like mine. So in keeping with the aphorism that “a picture is worth a thousand words,” I’ve decided to give a few brief vignettes in this post that I think better illustrate what I offer than any bullet-point list of services you’ll find elsewhere on my website.
A few weeks ago I was interviewed by Chris Habig at the Healthcare Americana podcast. The episode was released this morning, so if you have 30 minutes and want to hear me drone on about my practice, the benefits of direct primary care, what holistic medicine means to me, etc., click the link below:
Many patients want to lose weight, either for health or aesthetics reasons, and the question of “what’s the best diet?” is one I’m asked frequently.
I’ve evolved my thinking on this in my years in practice. When I first started out, I used to recommend low-carb diets very frequently. And indeed, low-carb diets can work amazingly well. Both in numerous studies and in my experience with patients, there are a wide variety of low-carb diets (Keto, atkins, paleo, etc) that often work wonders. I still think that these diets are a great way to go for many people.
But I’ve also seen plenty of countervailing studies and patients, with the most obvious example being those folks who go onto a high-carb vegetarian/vegan diet and also see terrific results.
Given this, when I’m asked about the best diet, my quickest answer is to advise people to follow the diet that they feel they are most likely to enjoy and be able to stick to. Even if, hypothetically, there was one particular diet that truly worked best with your unique biology, it would be of little use if you hated it and burned out on doing it after just a few weeks.
But my real answer goes even a step further: you don’t need to follow a rigid “diet” at all. Rather, it’s often easier and more sustainable to adopt specific lifestyle principles that you can stick to indefinitely. What are these principles?
Just before leaving office at the end of his second term, President Dwight Eisenhower gave a speech in which he famously warned of the “military-industrial complex.” By this he meant that having large military budgets year after year was creating a powerful class of business interests who viewed the American military not simply as an institution vital to national security, but rather as a source of their own financial profits, and would hence forever exert pressure on the US government to increase military spending, regardless of whether it was otherwise appropriate to do so. This critique – which was shocking at the time – in retrospect seems rather obvious. Most observers of the US government now agree that there is an important interplay between the congress, the military, and the armaments industry, and the idea of a “military-industrial complex” is widely taken for granted.
Sadly, I see many parallels to the military-industrial complex in America’s modern medical system. Such as the way that pharmaceutical companies give generous donations to congressional members, who then pass legislation that is favorable to those companies. Or how the regulators of the pharmaceutical industry often obtain plum jobs with the pharmaceutical companies once they leave government, thus giving them an incentive while in office to “play nice” with them. Or how a small cadre of doctors sit atop the leadership at places like the NIH, controlling where grant money for research will go, thus creating an environment in which research that counters those doctors’ preferred ideas or theories is much less likely to receive funding.
But I want to talk about one such “complex” that particularly irks me, which I hereby will call the “academic-media complex.”
This will be a VERY brief post. I just wanted to announce two things:
First off, our practice was featured this week in the local newspaper. Find a copy of the Sippican Week and turn to page 17, or else click here to read the story. Thanks to reporter Erez Ben-Akiva for taking the time to stop by the office and get to know us.
By way of reminder, this Sunday (June 30) we will be hosting an open house along with four other Marion businesses as part of the “Dose of Wellness” event. Feel free to drop by from 8am-12pm on Sunday to see the office, meet us, and have a complimentary body composition scan. You can read my prior blog post here for more details.
As I’ve often written on this blog, one of my motivations for leaving corporate medicine and starting my own boutique practice is the opportunity to work much more extensively with my patients on lifestyle and other “holistic” modes of care, rather than working in an environment where the time pressures and financial incentives are oriented towards treating every problem that comes my way with a pill. As I’ve also written, this is not because I think pills are always, and in all situations, bad, but rather because lifestyle is usually much more effective than pills for promoting health and longevity; because a healthy lifestyle has (unlike pills) no negative side effects; and because it gives me a more rounded set of tools with which to help my patients. But let me add another reason why it’s best to avoid pills when reasonably possible: medicine is a big business, and like all big business, sometimes prone to corruption.
So annoying, in fact, that I googled it, and found out that there’s a whole culture of people out there who find the ad equally repellent. Many, unfortunately, have commented on the size of the main actress, and the backlash against the backlash against the commercial (isn’t everything in America these days a backlash against a backlash?) is that the haters of the commercial are simply “fat shaming” the actress. So let me state right off the bat that indeed, fat shaming is a horrible thing, and my objection to the commercial has nothing to do with the fact that the lead actress is overweight.
Rather, what really irritates me about the commercial (other than the cloyingly obnoxious jingle) is that it perpetuates the great pharmaceutical lie about type 2 diabetes: namely, that it’s an incurable disease that is best controlled with medication. Nothing could be further from the truth. The fact is that type 2 diabetes is often curable, and almost always manageable, with lifestyle modification, and – provided they make the correct changes – many type 2 diabetics don’t require any medication at all.
In recent years, there has been an explosion of interest in healthcare related content on the internet. Podcasts by figures such as Peter Attia, Andrew Huberman, Rhonda Patrick, Ken Berry, and Gabrielle Lyon, to name a few, have become extremely popular. Typically these podcasts take a health issue and dissect it for the average person, often with a bit of a different perspective than is found in mainstream medicine. And while I don’t agree with every single thing that each of the above doctors says or touts, I think that overall these folks do a great service to the American (and global) public by empowering people to learn more about how to take charge of their own health.
I’m excited to announce that on Sunday, June 30, we will be participating in “A Dose of Wellness,” a multi-business open house here in Marion.
On that date, anybody in the community is welcome to drop by our office (no appointment needed) between 8:00 am and 12:00 noon to get a free tour of our office, meet me, and learn more about the practice. And, as an added bonus, anybody who comes in that morning will be given a free body composition scan with my Styku device (see image below for an example scan – for best results, wear tight/form fitting clothes). In addition, any visitors will be entered into a raffle for a complimentary red light treatment session.
V0027010 Ivan Petrovitch Pavlov. Photograph after a photograph taken
Credit: Wellcome Library, London. Wellcome Images
images@wellcome.ac.uk
http://wellcomeimages.org
Ivan Petrovitch Pavlov. Photograph after a photograph taken in 1934.
Published: –
Copyrighted work available under Creative Commons Attribution only licence CC BY 4.0 http://creativecommons.org/licenses/by/4.0/
The man pictured above is Ivan Petrovich Pavlov (1849-1936) and if you are wondering why the photo of a long deceased Russian scientist is adorning this post, read on. I’ll come back to it by the end – I promise.
In my last two posts (click here and here if you haven’t read them yet), I discussed some tips for developing the correct mindset towards sleep and to lessen the anxiety about sleep that is usually at the root of insomnia. If you suffer from chronic poor sleep, it’s really worth re-reading these posts and internalizing them before going further. With that said, today I’m going to change directions and start talking about steps you can take to actually start sleeping better.
This is part two of a series on how to sleep better. In my last post, I discussed how many people who complain of poor sleep are, in fact, already better sleepers than they think. I discussed how this was important to understand for two reasons: 1) because insomnia is often a self-perpetuating anxiety issue (we don’t sleep well and then start to stress about not sleeping well, which leads to not sleeping well, which leads to more stress about not sleeping well, and so on), and 2) because research indicates that just thinking you are a poor sleeper can in and of itself lead to feeling more tired and less focused during the day. I also promised that I would soon start giving some tips on how to actually sleep better. And I will. In a coming series of blog posts. But first, I really need to hit this point about anxiety a little bit more. Because, until you learn to stop stressing about your poor sleep, it’s going to be much harder to overcome your poor sleep.
My last few posts have revolved around nutrition and weight loss – a topic about which I am very passionate. Without a doubt, nutrition and exercise are two of the most important aspects of living a long and healthy life. But there is a third major pillar of good health about which patients frequently come to me for advice: how to sleep better.
In my last post, I reviewed a study that highlighted the beneficial effects of eating more protein. Today I want to review another study that highlights the benefits of limiting processed food in the diet.
In today’s blog post, I will briefly review a fascinating study that was first published in 2005, and that should inform our approach to losing weight and improving our fitness and metabolic health.
In my last post, I introduced our new body composition scanner, Styku. Today, I’m proud to announce that our second big piece of “bio-hacking” equipment is now fully functional here in the office: our Soleil-Well Red Light Device.
What is a red light device? It is, as its name implies, a device that shines very bright and powerful red (and near infrared) light onto the body. Truly it’s no more complicated than that – one simply stands in front of the device for a few minutes and allows the light to soak into their body. It’s completely painless, completely non-invasive, and virtually risk free, as it does not emit any radiation or ultraviolet light.
I’ve written a lot about the benefits of direct primary care to my patients. But here’s another one – unlike in my prior corporate job, I can actually take some time out of the office to recharge. Doctors are only human, and we actually perform our jobs with more intelligence, creativity, and compassion when we’re well rested and get to spend adequate time with our family and friends. Accordingly, I’m doing something this week that I’ve rarely done in my career as a physician before: closing shop in order to hang out with my kids, who have the week off from school for spring break.
We’ll be back in the office next Monday. Until then, my patients should feel absolutely free to text or call me for anything important. But otherwise I’ll be off, meaning no further posts to this blog nor uploads to our social media channels for the next seven days.
I am proud to announce that, several months after ordering it, our Styku body composition scanner arrived last week and is now operational. Starting immediately, my patients can regularly have painless, non-invasive, radiation free body scans here in the office that will provide them with key information about their metabolic health and their risk for developing chronic diseases such as diabetes, hypertension, and cancer, as well as feedback about weight loss and fitness efforts.
A few years ago, back when I was still an employee at a large corporate practice, a middle aged woman who I knew well came to see me complaining of abdominal pain. I took a history from her, examined her carefully, and reviewed her recent labs. After doing so, I was reassured that she had nothing serious going on and needed no further workup for the moment.
So I did exactly the sort of “irrational” thing that makes no sense to an insurance company but all the sense in the world to a doctor: I ordered an abdominal ultrasound.
The photo above is of John D. Rockefeller. The founder of the Standard Oil Company, he is considered by many historians to be the single richest human being who ever lived. Mr. Rockefeller was simultaneously a ruthless businessman and a very generous philanthropist, and is thus remembered as both a villain and a hero of American history. But for the purposes of this article, what’s relevant is that Mr. Rockefeller lived to the age of 97, and remained mentally sharp and physically active right up until almost the very end of his long life.
I’ve mentioned in a prior blog post that I’m a history buff and that I sometimes wonder whether we can learn anything from the past about better health habits. So it was that while reading a biography of Mr. Rockefeller a few years ago, I was struck by something – John D. Rockefeller was a devotee of circadian medicine, nearly a century before the field was even invented.
I’ll come back to John D. Rockefeller in a moment, but first: what is Circadian medicine?
In my last post, I touched on some factors other than diet and exercise that can impact your weight loss efforts.
Today I want to discuss three random studies. None of them have anything to do (at least not directly) with each other, and none of them represent “the” solution to weight loss. I highlight them rather to reinforce the point that, if you are paying attention to the ever expanding (no pun intended) science of obesity and weight loss, you should understand that eating more and moving less are only one part of the story.
One of my biggest interests – and one of the most common goals patients have – is weight loss. It’s also a common area of frustration. After all, it SHOULD be a simple thing. Change your diet and move more, right? What could be easier than that? And yet, millions of Americans try this approach every year, and most of the time it fails them. Why?
I bill myself as a “holistically minded” doctor. What I mean by this is not that I have any formal training in “holistic” care – I haven’t, for example, done a course in functional medicine, or in acupuncture. Rather, I have always had the bias that the human body is a wondrous and complex machine about which even we 21st century doctors know very little, and that many health problems can be either averted or healed if the body is simply given the optimal environment and left to do its own thing.
My last post was about the basic biology of insulin resistance and about how it is the underlying root cause of type 2 diabetes, as well as a risk factor in its own right for many diseases.
Today I’m going to answer the question of how to tell if you have insulin resistance.
Tens of millions of Americans suffer from insulin resistance, and most of them don’t even know it. Left unchecked, insulin resistance can lead to heart disease, cancer, dementia, type 2 diabetes, high blood pressure, and lots of other bad health outcomes. But before I can get into explaining how you can know if you have this condition, and what you can do about it if you do, I first need to explain what insulin resistance is.
I was a history major in college, and to this day one of my great interests outside of medicine is learning more about the past. Sometimes I even like to combine these interests by considering whether people of the past have anything to teach us about good health (they certainly have a lot to teach us about bad health in terms of death from things like infection, trauma, and childbirth, but that’s a fairly obvious point that you probably don’t need me to explain in detail).
Thus it was that about a year back, I was watching a documentary about the Roman empire and got to wondering: just how exactly did the Romans prepare their soldiers for combat?
This post is going to be relatively short, and may seem a bit frivolous, but I wanted to write it because it’s about a seemingly small thing that reveals a much deeper truth about DPC (Direct Primary Care) and how it differs from a traditional primary care setup.
Recently I purchased a Nespresso Vertuo machine for the office. I’m a bit of a coffee snob, and let me tell you – this thing makes amazingly delicious espressos.
This post will be extremely short. Back in October of 2023 – when I was still employed at my former practice – I was asked to give a lecture at a conference of physical therapists in Rhode Island. The theme of the conference was lifestyle (nutrition, exercise, sleep, etc.) and how it can positively impact joint health. The focus of my talk was on nutrition, with an emphasis on how proper nutrition can support better joint health and ease chronic pain, as well as on tips for losing weight. If you are interested, the folks who sponsored the conference have now posted a video recording of the talk on YouTube, embedded above.
Special bonus: if you forward to the 24:28 mark and watch just the last seven minutes of the video, you will hear my thoughts on what we can learn from the ancient Romans about how to have better health today – a topic that I will be returning to in another blog post soon.
There are so many problems with our current healthcare system. The difficulty getting appointments. The rushed visits. The paperwork. The surprise bills. I’ve addressed how Direct Primary Care solves a lot of these in my last post. But there’s another element I haven’t touched on yet, but that’s ultimately even more important: insurance driven care is very standardized, which means that it’s often five, ten, or even twenty years behind the science.
To illustrate this point, let me give an example. Let’s suppose that tomorrow a new test was developed that could accurately diagnose pancreatic cancer (one of the most lethal types of cancer) years before it could otherwise be detected by current means. You would think it would be adopted right away by the medical establishment and that doctors would be offering it to every patient at their annual physical starting immediately. But it’s almost certain that would not happen.






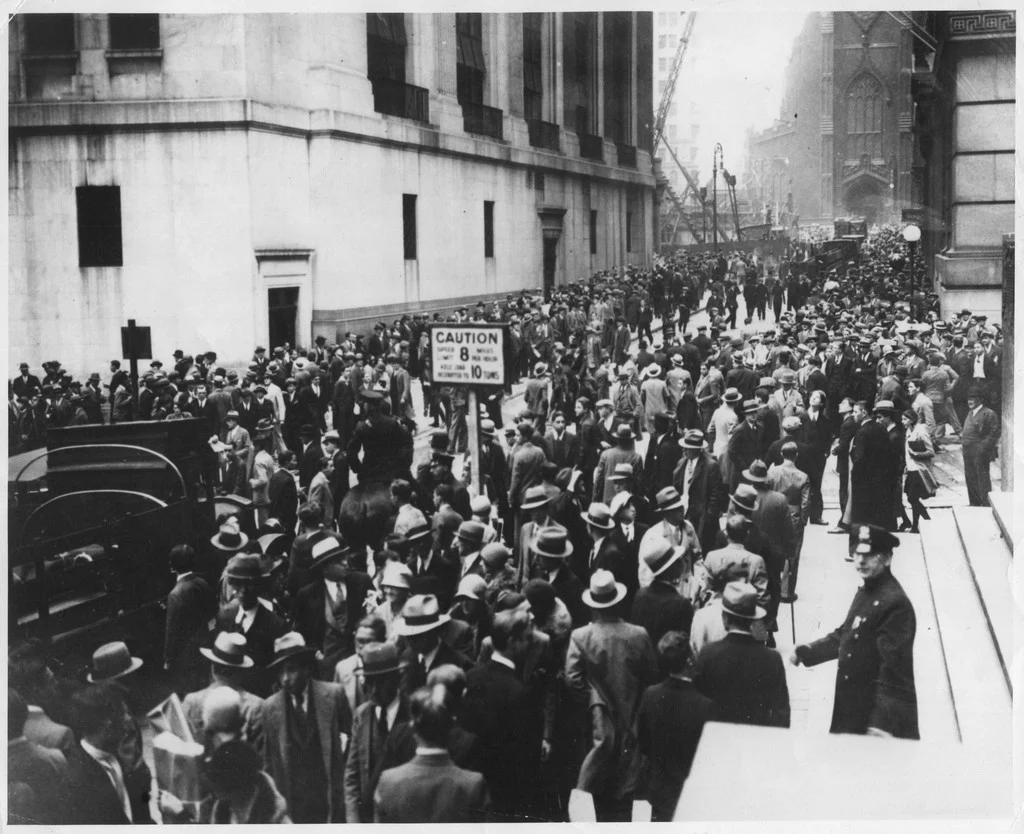



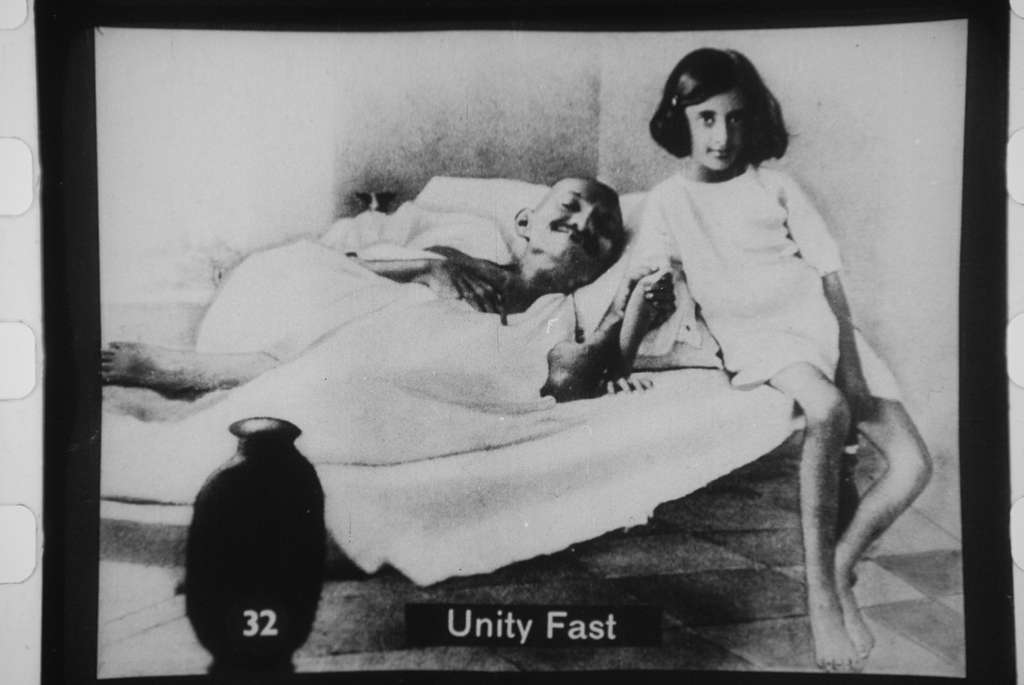
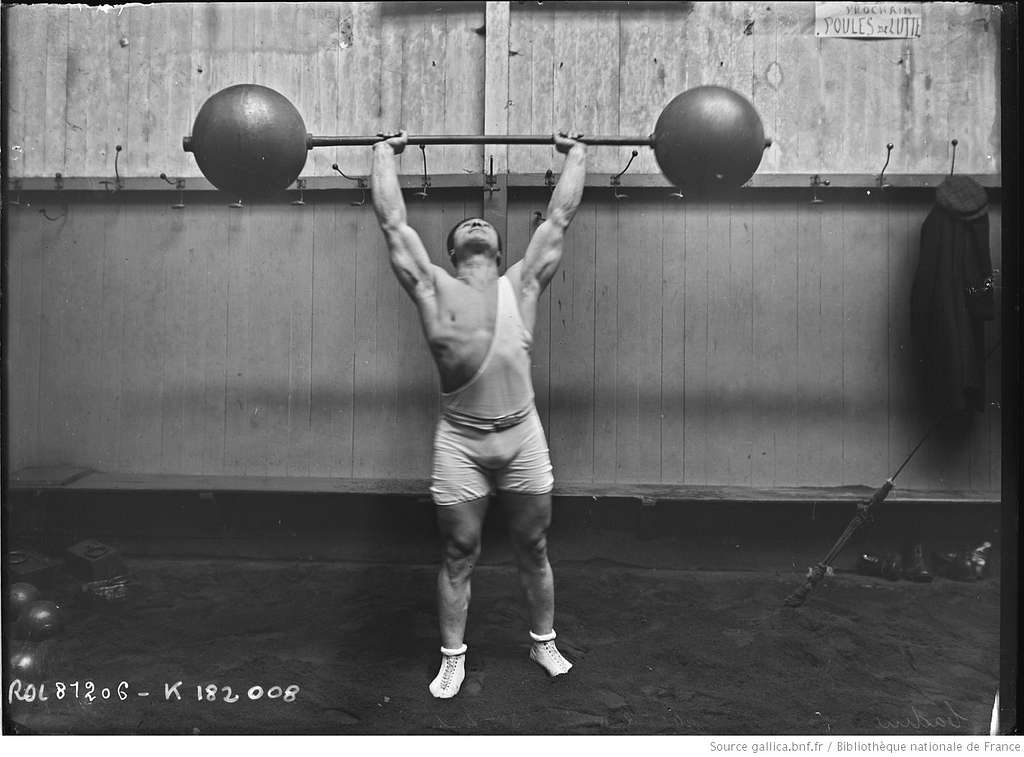



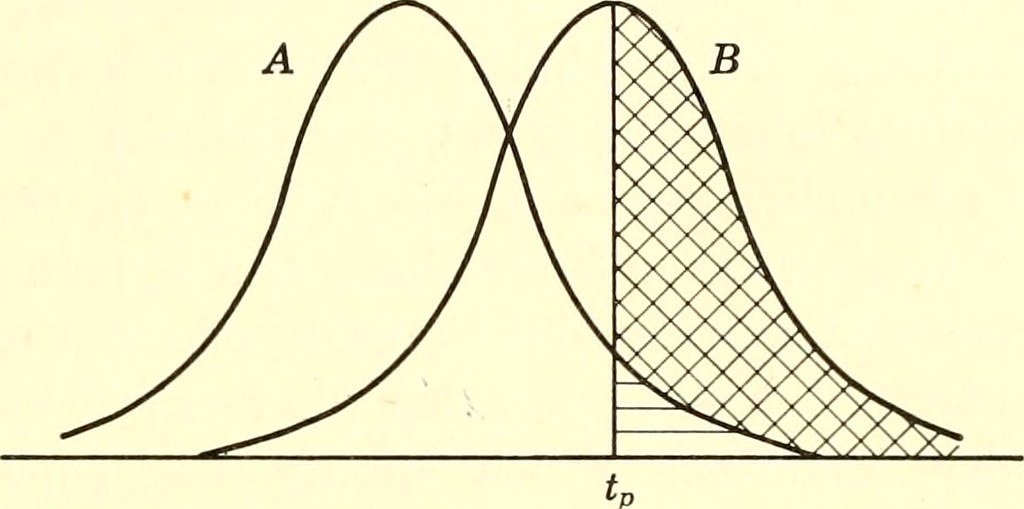














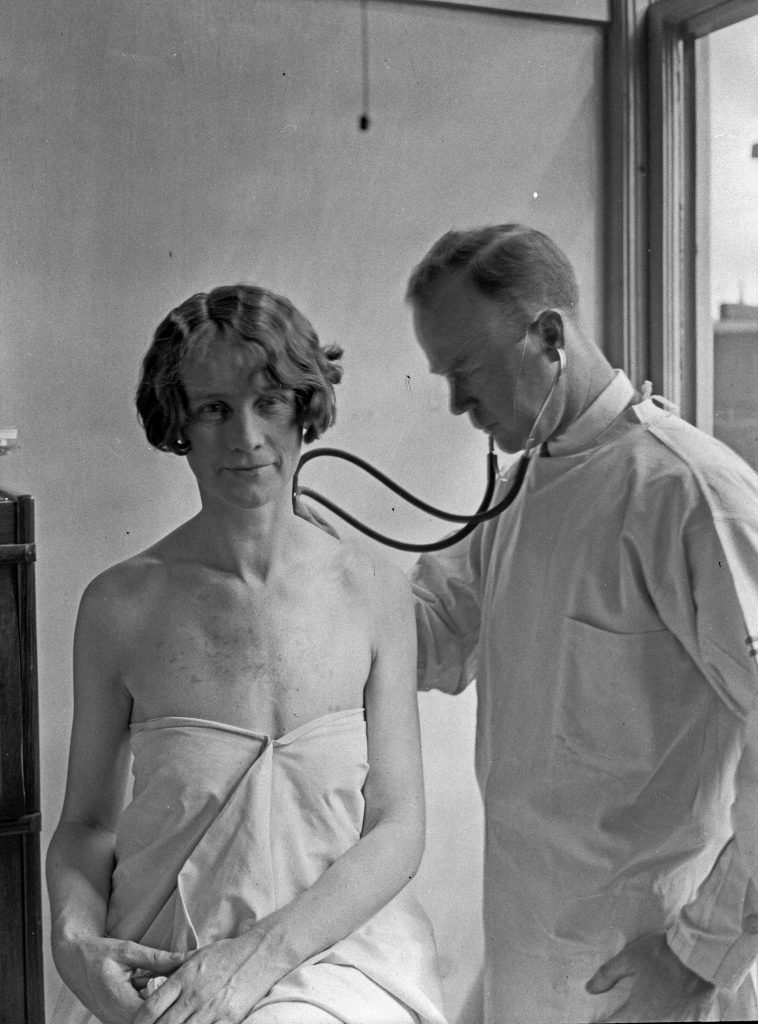



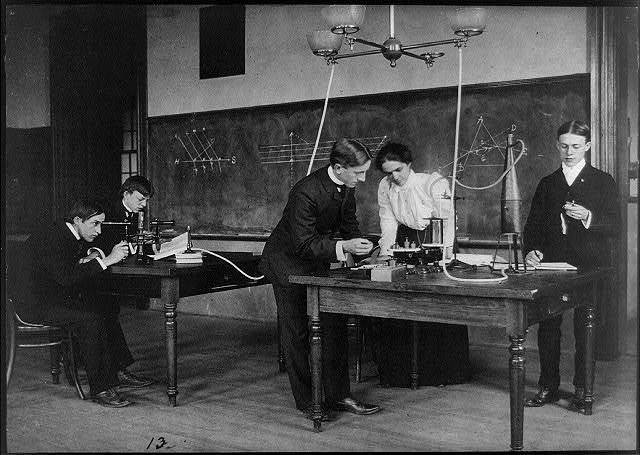









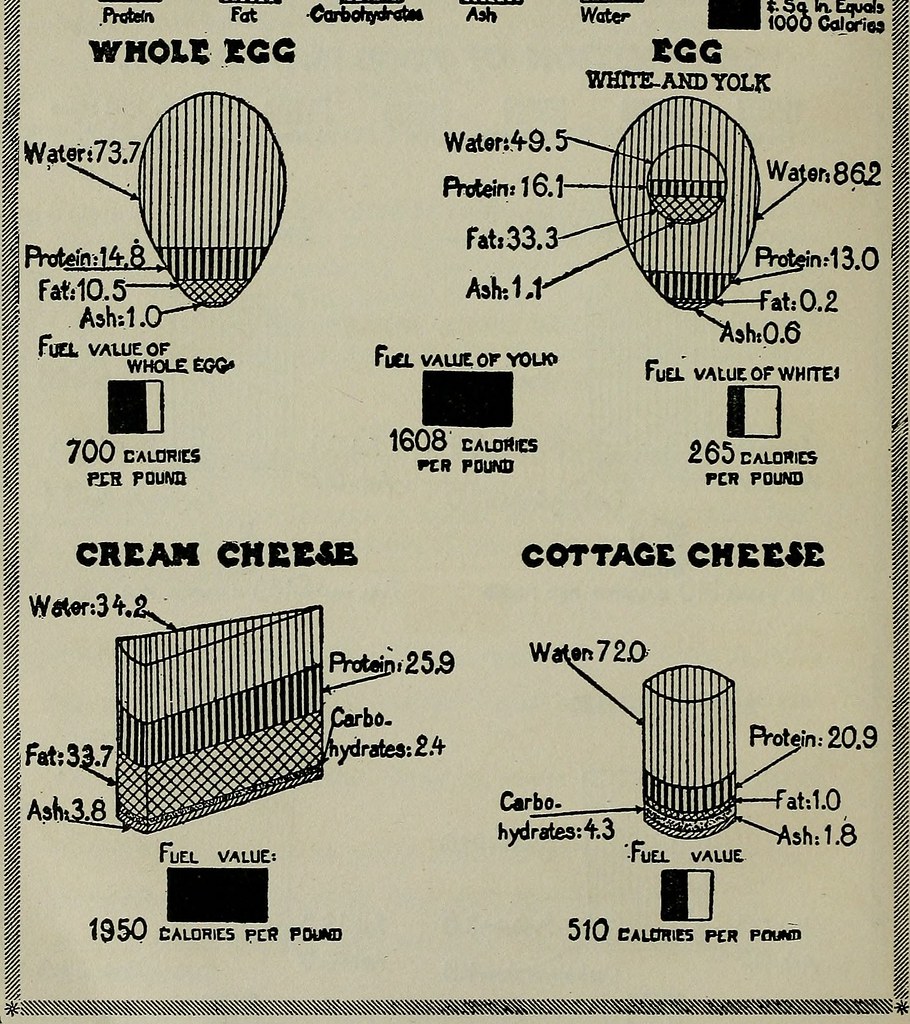













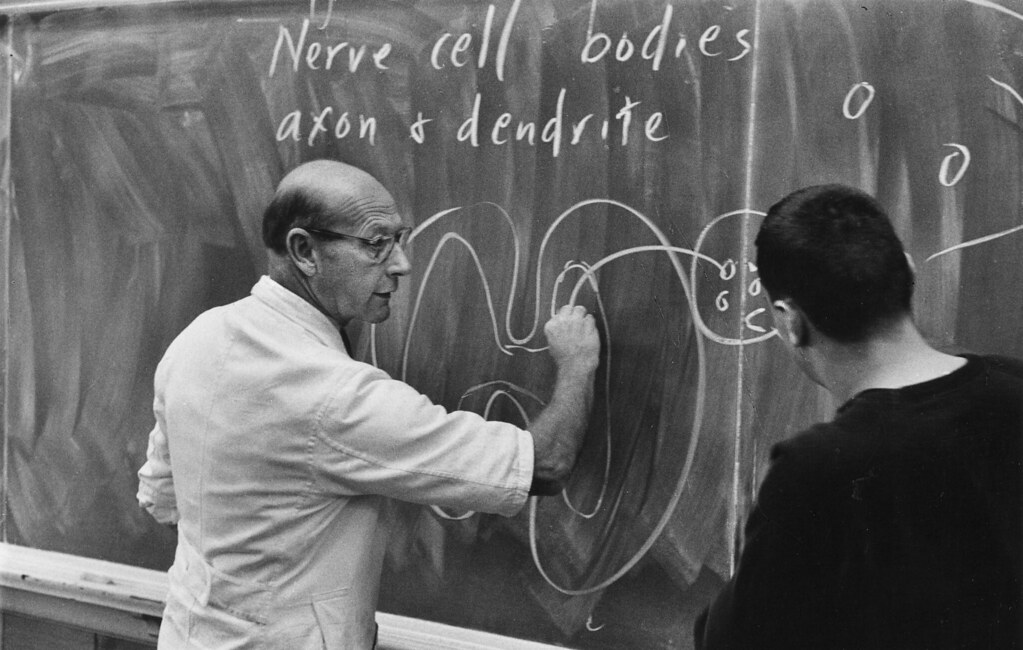
















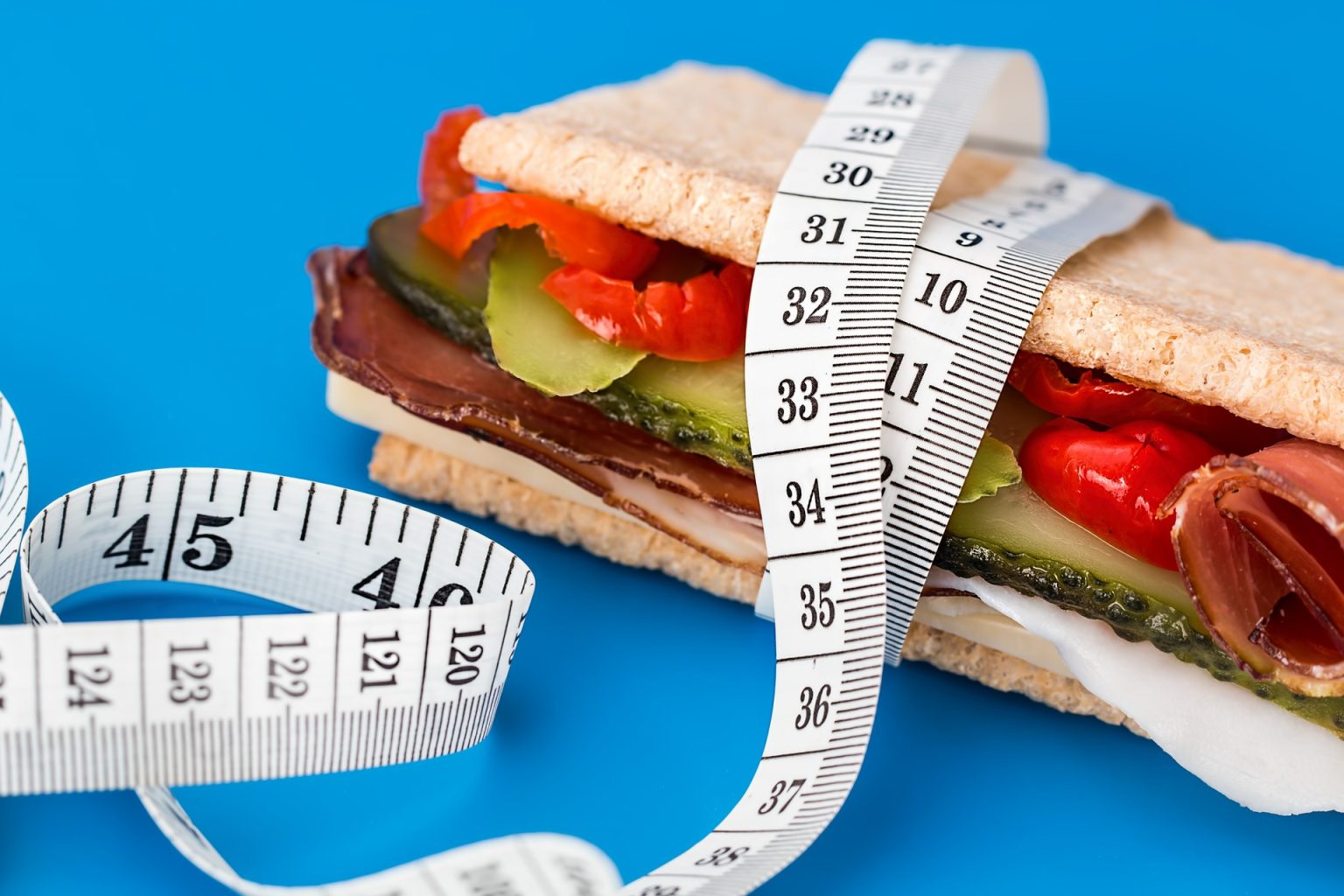











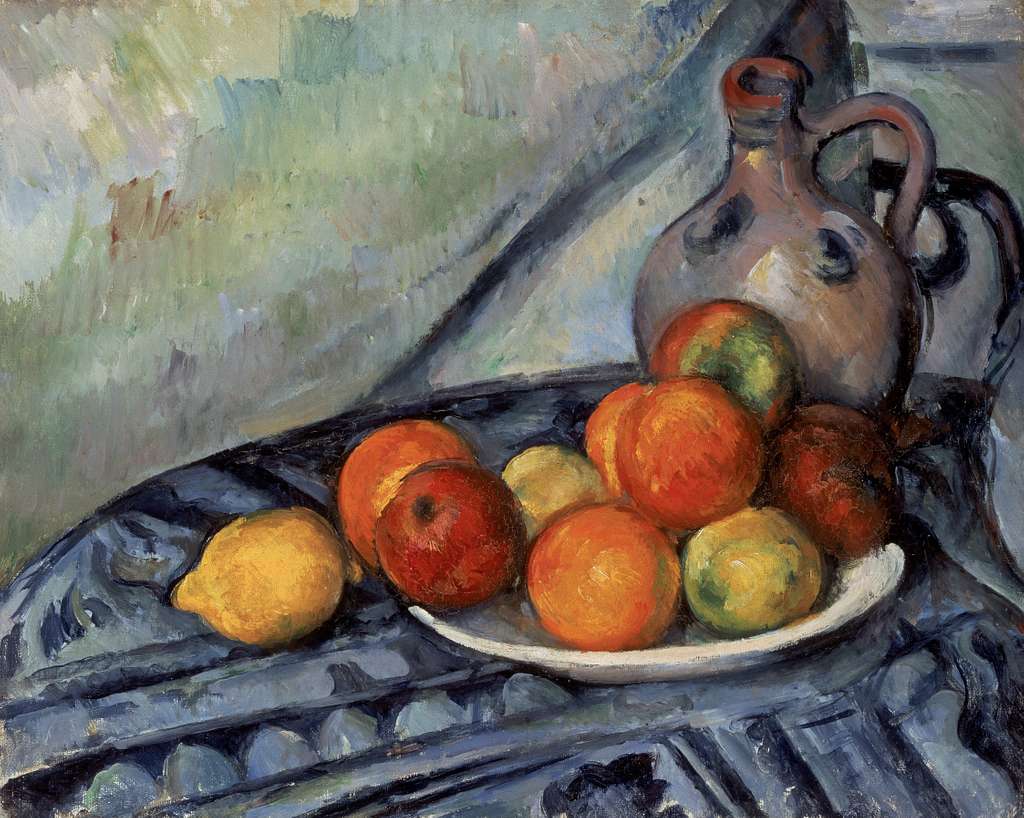








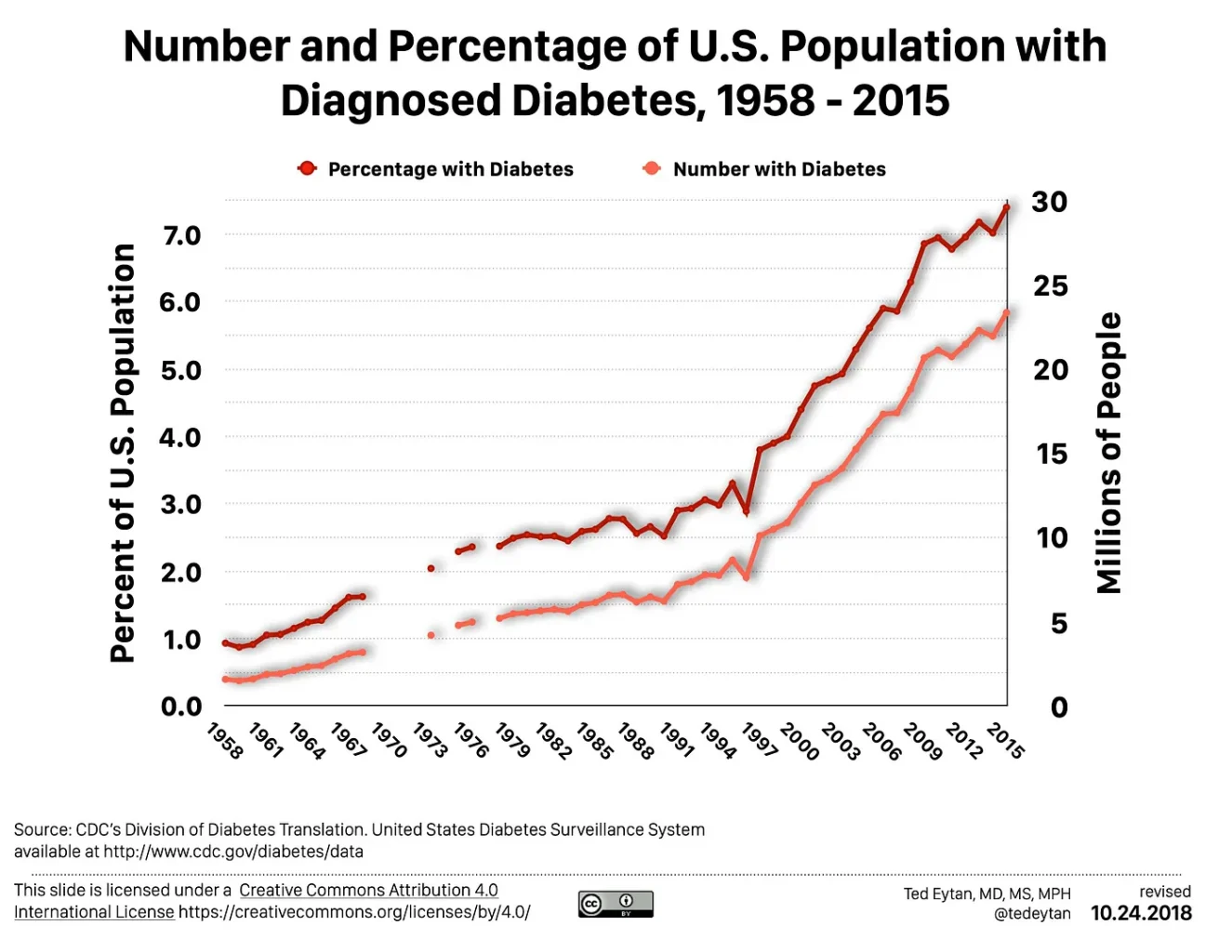




{kind=link}